Aquaculture & Quality Assurance
Breeding science, storage protocols, 6-point quality assessment, FDA requirements, and supply chain logistics for clinical-grade medicinal leeches.
Clinical Evidence — Not FDA-Evaluated
This page combines educational content on leech breeding biology and aquaculture science with regulatory guidance for FDA 510(k) compliance, OSHA Bloodborne Pathogen Standard adherence, and clinical storage protocols. Practitioners must verify current federal, state, and local regulations applicable to their jurisdiction. All medicinal leeches used in the United States must be sourced from FDA-cleared suppliers.
Chapter 2, Section 2.5 — Handling, Storage & Quality Assurance
Last updated: June 18, 2026
The clinical efficacy of medicinal leech therapy (Hirudo verbana, Hirudo medicinalis) depends fundamentally on leech quality. Unlike pharmaceutical agents manufactured under GMP conditions, medicinal leeches are living biological devices whose therapeutic properties — salivary anticoagulants, vasodilators, anti-inflammatory compounds — vary with genetics, rearing conditions, feeding history, and storage. Aquaculture of clinical-grade leeches represents the critical first link in the chain of therapeutic quality. This page traces that chain from 1852 through modern biofactory operations, reproductive biology, quality assessment, FDA regulatory requirements, OSHA workplace safety mandates, supply chain logistics, and infection prevention.
Aquaculture Overview
Aquaculture — the controlled breeding, rearing, and quality management of aquatic organisms — has been applied to medicinal leeches since the mid-nineteenth century. Wild harvesting of Hirudo medicinalis across Europe had driven populations to near-extinction by the 1840s, as peak hirudotherapy consumed an estimated 100 million leeches annually in France alone. Captive breeding offered a sustainable alternative, and the first systematic manual appeared in 1852 (Brakov).
Today, medicinal leech aquaculture is a regulated industry. In the United States, leeches intended for therapeutic use are 510(k)-cleared medical devices (unclassified pre-amendment category). Three suppliers hold valid clearance: Ricarimpex SAS (France), Biopharm UK Ltd. (UK), and Carolina Biological Supply Co. (USA). In Russia, OOO "Girudomed" in Lyubertsy operates one of the largest biofactories. The primary objective across all facilities: producing high-quality, highly active, clinical-grade leeches whose salivary gland secretion profiles meet therapeutic thresholds.
Modern aquaculture encompasses the entire life cycle: controlled mating, cocoon collection and incubation, threadling rearing with artificial blood meals, multi-month fasting periods, phenotypic quality screening, and rigorous pre-shipment quality assurance. Each stage has failure modes that directly affect clinical outcomes.
Key Aquaculture Parameters
| Parameter | Specification | Rationale |
|---|---|---|
| Species | Hirudo verbana (primary), H. medicinalis | Only species with FDA 510(k) clearance for clinical use |
| Breeding temperature | 18–22°C (winter), 24–27°C (summer) | Optimal cocoon deposition ranges (Sineva 1944) |
| Water quality | Dechlorinated, pH 6.5–8.0, low hardness | Phenotypic quality correlates with water chemistry (Garmash 2001) |
| Feeding source | Fresh bovine blood from healthy slaughterhouse animals | Nutritional adequacy for growth; eliminates disease transmission |
| Pre-clinical fasting | 3–6 months minimum | Ensures feeding motivation; maximizes salivary secretion volume |
| Clinical size range | 3–10 cm (Mumcuoglu 2014) | Below 3 cm: insufficient blood extraction. Above 10 cm: excessive wound size |
| Cycle time (egg to clinical) | 12–18 months (Sineva 1944) | Includes growth, multiple feedings, and final fasting period |
History of Captive Breeding
The systematic captive breeding of medicinal leeches has a documented history spanning over 170 years. Understanding this trajectory is essential for appreciating the scientific foundations of modern biofactory protocols.
Brakov 1852: The First Manual
Brykov (1852) published an early Russian manual for leech breeding and husbandry, establishing foundational protocols for environmental control, colony management, and feeding schedules. This early codification of leech aquaculture predates modern biofactories by over a century.
Sineva 1944: The Laboratory Breakthrough
M.V. Sineva (1944) was one of the pioneers — together with G. Shchogolev and M. Fedorova — of controlled captive breeding of Hirudo medicinalis, rearing leeches under laboratory conditions and obtaining viable offspring. The breeding parameters this group established still inform biofactory operations today:
- Temperature dependency: Cocoon deposition occurs at 18–22°C during winter periods and 24–27°C during summer, suggesting photoperiod-temperature coupling in reproductive triggers.
- Cocoon production: A single individual produces 3–8 cocoons per reproductive cycle, with each cocoon containing 18–25 eggs.
- Social dynamics: Prolonged cohabitation increases copulation frequency, but paradoxically, groups of 5–6 individuals deposit fewer cocoons than isolated pairs — suggesting competitive inhibition of reproduction at higher densities.
- Interbreeding: All recognized morphological forms interbreed readily and produce viable offspring, confirming conspecific status despite phenotypic variation.
Kuznetsov 1975 and Lukin 1976
Kuznetsov (1975) extended Sineva's work with detailed cocoon morphometry: 15–25 mm length, 16–17 mm width, spongy proteinaceous shell. Egg counts refined to 6–30+ per cocoon. Threadlings emerge at ~1 month, measuring 7–8 mm and weighing 0.02–0.03 g. Critically, jaw apparatus in threadlings is initially poorly developed, requiring months of growth before attaining the triradiate jaw structure capable of clinical blood extraction.
Lukin (1976) provided the authoritative taxonomic monograph for Hirudo, confirming annual summer cocoon deposition across the Eurasian range. His documentation of phenotypic plasticity — the same species displaying markedly different morphology in different water bodies — laid the groundwork for Garmash et al.'s (2001) environmental quality control studies.
Historical Continuity
Reproduction Biology
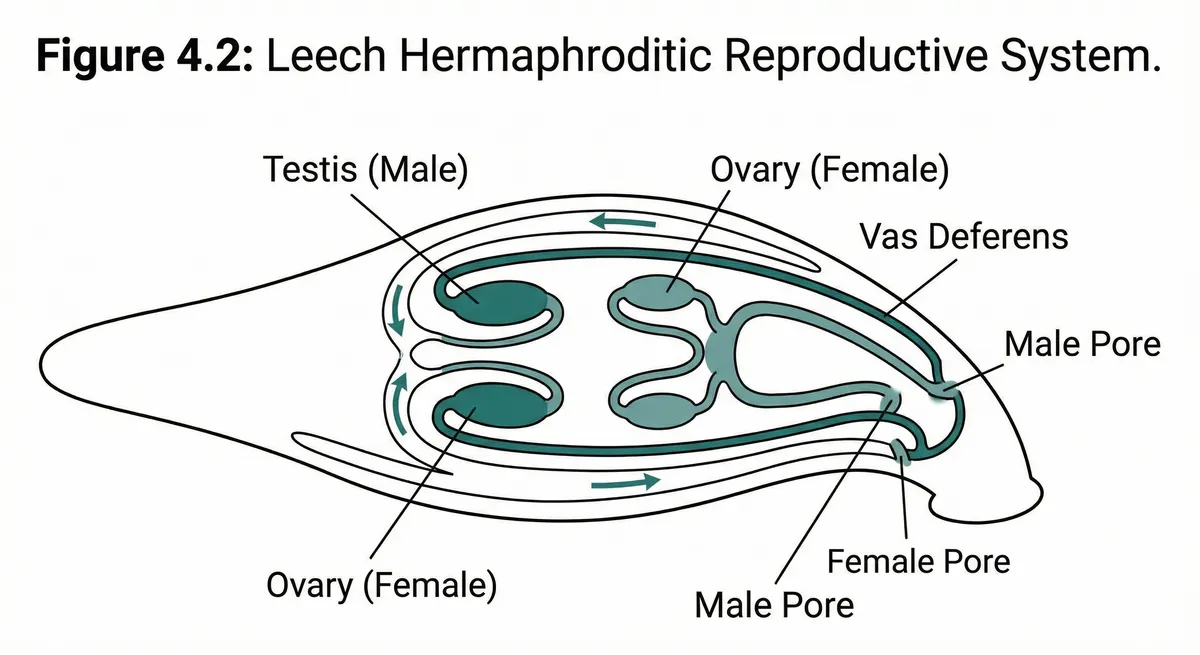
Medicinal leeches are simultaneous hermaphrodites but reproduce exclusively sexually, requiring copulation between two individuals. Self-fertilization does not occur. This obligate cross-fertilization has important implications for breeding program design.
Reproductive Cycle
- Mating: Two individuals align ventral surfaces and exchange spermatophores. Fertilization is internal. Prolonged cohabitation increases copulation frequency (Sineva 1944).
- Cocoon deposition: Once annually, during summer months. Optimal temperature 24–27°C (summer) or 18–22°C (winter under laboratory photoperiod manipulation).
- Cocoon morphology: Ovoid, 15–25 mm length × 16–17 mm width. Spongy shell composed of proteinaceous matrix secreted by the clitellum (Kuznetsov 1975).
- Egg count: 6–30+ eggs per cocoon (mean ~18–25 per Sineva; broader range per Kuznetsov).
- Per-individual output: 3–8 cocoons per reproductive cycle (Sineva 1944); 4–5 cocoons per individual (Kuznetsov 1975).
Juvenile Development
- Incubation: Approximately 1 month from cocoon deposition to juvenile emergence.
- Threadlings at emergence: 7–8 mm length, 0.02–0.03 g body weight. Translucent, with poorly developed jaw apparatus.
- Jaw development: The characteristic triradiate jaw with ~80 teeth per jaw (240 total) requires several months of growth post-emergence. Threadlings cannot perform clinical-grade bites.
- Growth to clinical size: 12–18 months from hatching to 3–10 cm clinical-ready size (Sineva 1944). Multiple feeding cycles with intervening fasting periods.
- Feeding transition: Threadlings initially fed on fresh bovine blood clots placed at container bottom. Later transition to whole-blood feeding.
Reproductive Output Estimates
| Parameter | Low Estimate | High Estimate | Source |
|---|---|---|---|
| Cocoons per individual | 3 | 8 | Sineva 1944 |
| Eggs per cocoon | 6 | 30+ | Kuznetsov 1975 |
| Eggs per individual (per cycle) | 18 | 240+ | Calculated range |
| Cocoon dimensions (L × W) | 15 × 16 mm | 25 × 17 mm | Kuznetsov 1975 |
| Threadling size at emergence | 7–8 mm, 0.02–0.03 g | Kuznetsov 1975 | |
| Time to clinical readiness | 12 months | 18 months | Sineva 1944 |
Social Density Effects on Reproduction
Sineva's (1944) observation that groups of 5–6 produce fewer cocoons than isolated pairs has practical biofactory implications. The mechanism likely involves pheromone-mediated reproductive inhibition at higher densities. Optimal breeding units: isolated pairs in dedicated containers, with pairing rotated for genetic diversity. Prolonged cohabitation of paired individuals increases copulation frequency, suggesting pairs should be maintained together for 4–8 weeks rather than briefly introduced.
Modern Biofactories
The global supply of clinical-grade leeches is concentrated in a small number of specialized biofactories integrating controlled-environment aquaculture, biosecurity, quality assurance, and regulatory compliance.
| Supplier | Location | Species | FDA Status | Key Details |
|---|---|---|---|---|
| Ricarimpex SAS | Eysines, France | Hirudo verbana | 510(k) cleared | Largest global supplier. European GMP-equivalent facility. Direct export to US hospitals. International cold-chain shipping network. |
| Biopharm UK Ltd. | Hendy, Wales, UK | Hirudo verbana, H. medicinalis | 510(k) cleared | Established 1812 lineage (claims oldest continuous leech supply). Supplies UK NHS and exports globally. Research-grade specimens also available. |
| Carolina Biological Supply Co. | Burlington, NC, USA | Hirudo verbana | 510(k) cleared | Only US-based supplier with FDA clearance. Also supplies educational/research specimens. Domestic shipping eliminates import logistics. |
| OOO "Girudomed" | Lyubertsy, Russia | Hirudo medicinalis | Not FDA-cleared (Russian market only) | One of the largest biofactories globally. Supplies Russian clinical market. Maintains large breeding colonies under controlled conditions. |
FDA Clearance Is Mandatory
Biofactory Operations Overview
Modern biofactories maintain colonies of thousands to tens of thousands of adults in climate-controlled systems, organized into sequential zones:
- Breeding zone: Isolated pairs in individual containers at optimal temperature ranges. Photoperiod manipulation to trigger reproductive cycling.
- Incubation zone: Cocoons collected and maintained in high-humidity incubators at 24–27°C for approximately 30 days until threadling emergence.
- Nursery zone: Threadlings reared in shallow containers with bovine blood clots. Multiple feeding cycles over 6–12 months.
- Growth zone: Adolescent leeches maintained under standard conditions with periodic feedings until reaching 3–10 cm clinical size range.
- Fasting zone: Clinical-ready leeches transferred to fasting containers. Minimum 3–6 months without food to ensure maximal feeding motivation and salivary output upon clinical use.
- Quality assurance zone: Pre-shipment assessment against 6-point quality criteria (see Quality Indicators section). Batch sampling for Aeromonas antibiotic sensitivity testing at high-volume facilities.
- Shipping zone: Packaging in moisture-retaining media (damp moss, hydrogel packs) with temperature stabilization for cold-chain transport.
Breeding Parameters
Parameters derived from Sineva (1944), Kuznetsov (1975), and Lukin (1976) form the evidence-based framework for modern biofactories.
Temperature Regimes
| Season / Phase | Temperature Range | Purpose | Duration |
|---|---|---|---|
| Winter maintenance | 18–22°C | Cocoon deposition (winter cycle) | Continuous during winter |
| Summer breeding | 24–27°C | Optimal cocoon deposition (summer cycle) | June–August in natural cycle |
| Incubation | 24–27°C | Cocoon development and threadling emergence | ~30 days |
| Nursery / growth | 20–24°C | Juvenile and adolescent growth with feeding | 6–12 months |
| Clinical storage / fasting | 18–22°C | Pre-clinical fasting and storage; reduces metabolic rate | 3–6+ months |
Cocoon Production Optimization
- Isolated pairs over groups: Individual pairs produce more cocoons than groups of 5–6 (Sineva 1944). Maximize output via many isolated pairs.
- Prolonged pairing: 4–8 weeks together increases copulation frequency and cocoon yield vs. brief introductions.
- Nutritional priming: Full blood meal 2–4 weeks before breeding season. Nutritional status affects cocoon capacity.
- Genetic rotation: Rotate pairs across seasons to prevent inbreeding depression in closed colonies.
- Post-deposition care: Cocoons collected intact and transferred to dedicated incubation chambers.
Feeding in Captivity
In nature, Hirudo species feed on amphibian, mammalian, and avian blood. In captivity, feeding must support growth and reproductive capacity while maintaining food safety standards.
Modern Bovine Blood Method
The standard biofactory feeding protocol uses fresh bovine blood obtained from healthy slaughterhouse animals. The blood is collected under sanitary conditions and used within 24–48 hours of collection to maintain nutritional quality.
- Threadling feeding: Coagulated blood clots are placed at the bottom of shallow containers. Threadlings feed by piercing the clot surface with their developing jaws.
- Adolescent feeding: Whole blood presented in membrane-covered containers that simulate host skin. Leeches bite through the membrane to access blood.
- Frequency: 2–4 feedings during the growth phase, with intervals of weeks to months between meals (leeches digest slowly over 4–6 months).
- Final fast: After reaching clinical size (3–10 cm), leeches are maintained without food for 3–6 months minimum to render them suitable for therapy. This ensures maximum feeding motivation and salivary output.
Historical: Lohner 1915 Glass Tube Method
In 1915, Lohner described an elegant artificial feeding technique using a glass tube apparatus:
- Apparatus: Glass tube with one end sealed by a thin membrane of mammalian skin (typically bovine or porcine intestinal membrane).
- Contents: Tube filled with mammalian serum at body temperature (~37°C).
- Mechanism: Leeches bite through the skin membrane and feed on the warmed serum. The skin membrane simulates the tactile and chemical cues of a live host.
- Significance: This was the earliest documented method for feeding leeches without access to a live host animal. Preceded the modern bovine blood clot method by decades.
While no longer used in commercial biofactories, the Lohner method established the principle that artificial feeding can sustain captive colonies indefinitely — a prerequisite for commercial aquaculture.
Food Safety in Leech Feeding
Phenotypic Quality Control
Garmash et al. (2001) demonstrated that Hirudo medicinalis populations from different water bodies display distinct phenotypes (body size, coloration, stripe definition, muscular tone, activity levels) correlating with environmental parameters:
| Environmental Variable | Effect on Phenotype | Clinical Relevance |
|---|---|---|
| pH | Acidic conditions (<6.5) reduce growth rate and darken coloration; alkaline (>8.0) increases stress mortality | Optimal pH 6.5–8.0 produces specimens with best vigor and feeding response |
| Water hardness | Hard water correlates with firmer body tone and more defined dorsal stripe patterns | Body tone is a key quality indicator; standardized hardness supports consistent quality |
| Temperature intervals | Chronic exposure to extremes (<10°C or >30°C) produces sluggish, smaller specimens | Maintained at 18–22°C, leeches exhibit optimal vigor, size, and feeding readiness |
| Dissolved oxygen | Hypoxic conditions increase surface-seeking behavior and reduce body tone | Adequate aeration essential for maintaining firm, elastic body tone |
| Organic load | High organic contamination increases disease susceptibility and integument lesions | Clean water with regular changes (every 48h) prevents integument compromise |
Biofactory water chemistry must be standardized and continuously monitored. Facilities drawing water from different sources across seasons may produce phenotypically variable stock, leading to inconsistent clinical outcomes. Environmental control is not merely a husbandry concern but a clinical quality assurance imperative.
Phenotype vs. Genotype
Clinical Storage Protocols
Proper storage at the clinical facility is essential for maintaining viability and therapeutic efficacy. Protocols below derive from Mumcuoglu et al. (2014) and institutional best practices.
| Parameter | Specification | Rationale | Failure Mode |
|---|---|---|---|
| Water type | Dechlorinated, 18–22°C | Chlorine is lethal; age tap water 24h+ or treat | Acute toxicity, death within hours |
| Water changes | Every 48h minimum; 72h maximum | Ammonia/mucus excretion degrades quality rapidly | Ammonia buildup: integument damage, lethargy, infection |
| Container | Glass (preferred) or food-grade plastic; 1–3L wide-mouth | Glass is inert; non-food plasticizers leach toxins | Chronic toxicity and phenotypic degradation |
| Lid | Mesh/perforated lid or 4-layer gauze + rubber band | Air exchange; leeches are strong escape artists | Sealed: hypoxia/death. Open: escape/desiccation |
| Light | Dark/dim area; no direct sunlight | Negative phototaxis; chronic light = stress | Agitation, escape attempts, reduced feeding readiness |
| Density | Max 10 per liter | Overcrowding: ammonia, abrasion, stress | Aggression, lesions, cannibalism |
| Fed/unfed separation | Strictly separate fed from fasting leeches | Fed release enzymes; unfed may cannibalize | Colony loss through cannibalism |
| Handling | Blunt forceps + nitrile gloves; never bare hands | Skin oils/soaps deter attachment | Contamination reduces clinical attachment |
| Aromatics | No perfumes, cleaners, sanitizer near storage | Sensitive chemoreceptors; volatiles = stress | Renders leeches unusable (non-attachment) |
| Shelf life | Use within 30 days of receipt | Prolonged storage degrades salivary output | Reduced vigor and lower therapeutic efficacy |
Daily Viability Check (Mandatory)
Quality Indicators: 6-Point Assessment System
A standardized 6-point quality-assessment framework is used at biofactories for pre-shipment screening and at clinical facilities for pre-application verification. All six criteria must be satisfied before patient use.
| # | Criterion | Pass (Acceptable) | Fail (Reject) | Assessment Method |
|---|---|---|---|---|
| 1 | Vigor | Active sinusoidal swimming; rapid response to light, vibration, warmth | Sluggish; absent stimulus response; resting at bottom | Agitate container; present warm gloved hand near surface |
| 2 | Body tone | Firm, elastic, smooth; rapid contraction when lifted with forceps | Flaccid, limp, bloated; minimal muscular response | Lift briefly with blunt forceps; assess tone |
| 3 | Coloration | Olive-green dorsal with orange-yellow stripes; lighter ventral | Pale, washed-out, or uniformly dark; absent stripes | Visual inspection under adequate lighting |
| 4 | Feeding readiness | Congregate at water's edge; orient toward warmth/movement | Hide deep; no interest in warmth; bloated abdomen | Present warm stimulus; hungry leeches orient within seconds. Use only fasting leeches |
| 5 | Intact integument | Smooth, uniform skin; no lesions, patches, or cuticle constrictions | Lesions, white patches (fungal), mucus coating, swelling | Inspect dorsal/ventral surfaces; check for segmental constrictions |
| 6 | Appropriate size | 3–10 cm relaxed length; proportional width | <3 cm: insufficient extraction. >10 cm: excessive wound | Measure relaxed (not contracted); most use 5–8 cm |
Pre-Shipment (Biofactory)
10% batch sampling against all 6 criteria. Batches with >5% failure held or culled. Document batch number, date, assessor, and pass/fail ratio.
Upon Receipt (Facility)
Inspect for shipping stress. Active/responsive within 1–2 hours of transfer. Record DOA count, shipment condition, and initial quality assessment.
Pre-Application (Point of Care)
Verify all 6 criteria for each leech before application. Any single failure = rejection. Document in procedure record.
FDA Regulatory Requirements for Medical-Grade Leeches
FDA-Cleared Indication
The following section describes binding federal regulatory requirements for the clinical use of medicinal leeches in the United States. These requirements apply to all practitioners, facilities, and suppliers. Non-compliance exposes practitioners and institutions to FDA enforcement action, OSHA citations, and malpractice liability.
510(k) Classification
Medicinal leeches are 510(k)-cleared medical devices (unclassified pre-amendment category) for US distribution — cleared based on substantial equivalence to a legally marketed predicate device.
FDA-Cleared Suppliers (Current as of 2026)
| Supplier | Location | Notes |
|---|---|---|
| Ricarimpex SAS | Eysines, France | International import; cold-chain shipping required |
| Biopharm UK Ltd. | Hendy, Wales, UK | International import; cold-chain shipping required |
| Carolina Biological Supply Co. | Burlington, NC, USA | Domestic supplier; eliminates import logistics |
Five Core Regulatory Requirements
- FDA-cleared source: Leeches must come from a 510(k)-cleared supplier. Verify clearance annually. Non-cleared sources (pet stores, bait shops, educational suppliers without 510(k)) violate federal law.
- Single-use mandate: One patient only, destroyed after use. No sterilization method renders a used leech safe for reuse.
- Biohazard waste: OSHA BBP Standard (29 CFR 1910.1030). Kill in 70% ethyl alcohol. Labeled biohazard containers. Final disposal per state/local regulations.
- Universal precautions: Written Exposure Control Plan. PPE: nitrile/latex gloves, forceps, gowns, eye protection for splash risk.
- Documentation: Number of leeches, application site(s), attachment duration, antibiotic prophylaxis (agent/dose/duration), and monitoring plan. Part of permanent medical record.
Practitioner Compliance Checklist
Biohazard Waste Disposal
Used medicinal leeches are regulated under the OSHA Bloodborne Pathogen Standard (29 CFR 1910.1030). While the standard contains no leech-specific provisions, blood-fed leeches are contaminated with potentially infectious material and fall under general requirements for handling, containment, and disposal of blood-contaminated items.
Kill and Disposal Protocol
| Step | Action | Specification | Rationale |
|---|---|---|---|
| 1 | Euthanize used leech | Immerse in 70% ethyl alcohol; maintain until complete cessation of movement (2–5 minutes) | Ethanol kills the leech and reduces pathogen load; 70% concentration is optimal for tissue penetration |
| 2 | Transfer to biohazard container | Red, leak-proof container with biohazard symbol; closable lid; rigid enough to prevent puncture | OSHA 29 CFR 1910.1030(d)(4)(iii)(A) requires that regulated waste be placed in containers that are closable, labeled, and leak-proof |
| 3 | Label and segregate | Container labeled with biohazard symbol and date; stored in designated biohazard waste area | Compliance with OSHA labeling requirements; prevents accidental contact by cleaning or maintenance staff |
| 4 | Contracted disposal | Licensed medical waste hauler; incineration or autoclave treatment per state/local regulations | OSHA regulates workplace handling but not final disposal pathway; state environmental agencies govern final treatment method |
OSHA Exposure Control Plan Requirements
Under 29 CFR 1910.1030, employers whose employees have occupational exposure to blood must maintain a written Exposure Control Plan:
- Exposed classifications: Physicians, nurses, medical assistants, and housekeeping staff who handle leeches or clean procedure areas.
- Exposure determination: Leech application, wound care, euthanasia, container cleaning, and biohazard waste transport.
- Engineering controls: Forceps (never bare hands), designated handling areas, splash-guard containers for euthanasia, impervious surfaces.
- PPE: Nitrile/latex gloves for all handling; gowns if splash risk; eye protection during euthanasia or removal.
- Annual review: Plan reviewed yearly, including evaluation of safer devices and procedures.
Jurisdiction Split
Supply Chain Logistics
All three FDA-cleared suppliers are located outside the contiguous United States (Ricarimpex in France, Biopharm in the UK) or within the US (Carolina Biological in North Carolina). This geographic distribution creates unique supply chain challenges that practitioners must address to maintain uninterrupted leech availability.
International Shipping Challenges
- Cold-chain: Maintain 10–22°C during transit. Excursions (<5°C or >30°C) cause mortality or quality degradation.
- Transit time: France/UK → US: 2–5 business days via expedited freight plus customs clearance.
- Import regulations: USDA APHIS compliance required for live animal import; state agricultural inspection may apply.
- Seasonal windows: Summer heat and winter freezes restrict shipping periods for some suppliers.
- Arrival condition: Must arrive alive, vigorous, fasting. DOA rates: 2–10% depending on conditions.
Supply Continuity Strategies
- Standing agreements: Recommended for institutions using >10/month. Pre-negotiated pricing and scheduled shipments.
- Dual sourcing: Maintain accounts with at least two FDA-cleared suppliers for backup.
- Buffer inventory: Rolling 2–4 weeks'' supply; leeches viable up to 30 days under proper storage.
- Domestic preference: Carolina Biological (NC) eliminates import logistics but may have limited availability.
- Emergency procurement: Pre-approved overnight delivery accounts for urgent microsurgical cases.
Supply Chain and Clinical Outcomes
Antibiotic Prophylaxis in Context
The connection between leech aquaculture and antibiotic prophylaxis is biological. Aeromonas hydrophila and A. veronii are obligate endosymbionts in the leech crop (digestive tract), producing hemolytic enzymes that aid blood digestion. These bacteria are not contaminants — they are essential to leech biology, present in every Hirudo verbana specimen regardless of rearing conditions.
Aeromonas as Obligate Endosymbionts
- Function: Aeromonas produce proteases and hemolysins that break down ingested blood, enabling nutrient absorption.
- Persistence: Colonization established during first blood meal, maintained lifelong. Biofactory hygiene cannot eliminate gut symbionts.
- Pathogenicity: Beneficial to leeches but pathogenic to humans — wound infections, cellulitis, and (rarely) sepsis.
- Infection rate: 2.4–20% without prophylaxis (de Chalain 1996; Lineaweaver 1992; Whitaker 2012). Onset 24h to >10 days.
Prophylaxis Protocols
Mumcuoglu et al. (2014) recommend fluoroquinolone (e.g., ciprofloxacin 500 mg BID) or trimethoprim-sulfamethoxazole (TMP-SMX DS BID) prophylaxis for all patients receiving leech therapy. Prophylaxis should begin before the first leech application and continue for 3–5 days after the last application.
First-Line Prophylaxis
- Ciprofloxacin: 500 mg PO BID
- TMP-SMX: DS (160/800 mg) PO BID
- Dual therapy: Cipro + TMP-SMX recommended by Herlin et al. (2017) as "most relevant" regimen
- Duration: Start before first application; continue 3–5 days after last leech
Critical Considerations
- Mandatory: Prophylaxis is not optional. Patients refusing antibiotics should not receive leech therapy (Mumcuoglu 2014)
- Resistance: Ciprofloxacin resistance up to 43% in some batches. Batch surveillance recommended for high-volume institutions
- Prophylaxis highly effective: standardized antibiotic prophylaxis markedly reduces leech-associated infection rates when applied consistently
- Without prophylaxis: 4–20% infection rate; infection markedly lowers flap-salvage success (Whitaker et al. 2011)
Patients Refusing Antibiotics
Mechanical Alternatives to Medicinal Leeches
Mechanical alternatives exist primarily for microsurgical venous congestion management where live leeches are unavailable, contraindicated, or refused by the patient.
| Device | Mechanism | Advantages | Limitations |
|---|---|---|---|
| Vacuum suction devices | Low-pressure vacuum applied to congested tissue; creates controlled blood evacuation through stab incision | No Aeromonas risk; no antibiotic prophylaxis needed; reusable; available on demand | No salivary compound injection (hirudin, hyaluronidase, vasodilators); purely mechanical blood removal; requires nursing for continuous operation |
| Chemical leeching | Heparin-soaked gauze applied to stab incision at congested site; maintains blood flow through chemical anticoagulation | No live organism required; predictable dosing; no infection risk from device | No vasodilation, no anti-inflammatory compounds; systemic heparin effects; requires frequent gauze changes; less effective than biological leeches |
| Pin-prick bleeding | Serial needle punctures to congested tissue to promote continuous low-volume blood egress | Immediately available; no special equipment; no infection from device | Labor-intensive; traumatic; no anticoagulant or vasodilator effect; inferior volume evacuation; not scalable |
The fundamental limitation of all mechanical alternatives is the absence of the leech's pharmacological payload. Biological leeches inject 100+ bioactive compounds including hirudin (direct thrombin inhibitor), hyaluronidase (tissue spreading factor), calin (collagen adhesion inhibitor), and histamine-like vasodilators. Mechanical blood removal cannot replicate this sustained local pharmacological environment. Biological leeches remain the gold standard for venous congestion management in microsurgery, and — unlike mechanical substitutes, which only address surgical congestion — are the only leech-based option applicable to non-surgical uses such as musculoskeletal pain and osteoarthritis, where leech therapy is used as one complementary modality among many.
Evidence Summary
The following table summarizes the key studies informing aquaculture science, quality assurance, and regulatory frameworks for medicinal leech therapy. Evidence spans foundational breeding studies, phenotypic research, expert consensus guidelines, and clinical infection data.
| Study | Design | Population (n=) | Intervention | Key Outcome | Result |
|---|---|---|---|---|---|
| Sineva MV 1944 | Laboratory breeding study | <em>Hirudo medicinalis</em> reared under controlled laboratory conditions (n=NR) | Complete life-cycle captive breeding over 12-18 months | Viable offspring generation; reproductive parameter documentation | Cocoons at 18-22°C (winter) / 24-27°C (summer). 3-8 cocoons per individual, 18-25 eggs each. Groups of 5-6 deposit fewer cocoons than isolated pairs Foundational study. All morphological forms interbreed readily. Basis for modern biofactory protocols |
| Kuznetsov BI 1975 | Reproductive biology study | <em>Hirudo medicinalis</em> from natural water bodies and laboratory colonies (n=NR) | Cocoon morphology, egg counts, temperature optima, and juvenile development documentation | Reproductive parameter dataset for captive breeding optimization | Cocoon 15-25 mm × 16-17 mm, spongy proteinaceous shell. 4-5 cocoons/individual, 6-30+ eggs each. Threadlings at ~1 month: 7-8 mm, 0.02-0.03 g Extended Sineva with quantitative cocoon morphometry. Jaws poorly developed in threadlings |
| Lukin EI 1976 | Taxonomic and ecological monograph | All known Hirudo species across Eurasian distribution range (n=NR) | Systematic documentation of biology, ecology, reproduction, and phenotypic variation | Authoritative taxonomic reference for genus Hirudo | Confirmed annual summer cocoon deposition. Phenotypic plasticity across water bodies. Validated interbreeding among forms Definitive Russian-language monograph. Still cited for reproductive biology and phenotypic data |
| Garmash SA et al. 2001 | Phenotypic comparison study | H. medicinalis populations from water bodies with distinct hydrochemical parameters (n=NR) | Morphometric/phenotypic analysis correlated with water chemistry (pH, hardness, temperature) | Phenotypic variation patterns and environmental determinants | Different water bodies produce distinct phenotypes. pH, hardness, and temperature favor particular characteristics Key for biofactory QC: standardized water chemistry necessary for consistent clinical-grade stock |
| Mumcuoglu KY et al. 2014 | Expert consensus + literature review | Practitioners of medicinal leech therapy across all indications (n=NR) | Comprehensive clinical recommendations: selection, quality assessment, storage, application, disposal | Standardized best-practice guidelines for all phases of leech use | 6-point quality assessment, storage at 18-22°C, water changed q48h, single-use mandate, fluoroquinolone/TMP-SMX prophylaxis Most-cited procedural reference. Established the quality indicator framework adopted worldwide |
| Lohner L 1915 | Experimental feeding study | Captive H. medicinalis requiring artificial feeding (n=NR) | Glass tube with mammalian skin membrane containing serum; artificial feeding without live host | Viability of artificial feeding for captive colony maintenance | Successful artificial feeding demonstrated; adequate nutrition without live host access Earliest documented artificial feeding technique. Preceded modern bovine blood protocols |
| Whitaker et al. 2012 | Systematic review | Plastic/reconstructive surgery patients, 67 publications (1966-2009) (n=277) | Leech therapy with variable prophylaxis (79% received antibiotics) | Infection rate, salvage rate, complication rate | 14.4% infection rate; infection markedly reduces flap-salvage success; 49.75% transfusion rate Landmark review. Prophylaxis adherence correlates with salvage outcomes |
| Lineaweaver et al. 1992 | Multicenter case series | Replantation/flap patients with post-leech Aeromonas infection (n=10) | Documentation of Aeromonas infections across surgical centers | Infection onset timing, severity, and tissue outcomes | Onset 24h to >10 days; severity from minor wound to tissue loss/sepsis Established mandate for routine antibiotic prophylaxis |
| Nguyen et al. 2012 | Prospective case series | 39 patients with standardized universal prophylactic protocol (n=39) | Standardized prophylaxis for all patients before leech application | Aeromonas infection rate under universal prophylaxis | 0% infection rate (0/39) Standardized prophylaxis eliminates clinical Aeromonas infections |
| Brakov NE 1852 | Technical manual | H. medicinalis in artificial captive breeding facilities (n=NR) | An early published manual on commercial leech husbandry | Feasibility of systematic captive leech breeding | Established foundational protocols: environmental controls, feeding schedules, colony management Earliest published manual on commercial leech farming |
Evidence Gaps & Research Priorities
Despite over 170 years of leech aquaculture history, significant knowledge gaps remain. The following areas represent priority targets for future research.
Aquaculture & Breeding Science
- Genomic standardization: No GWAS linking leech genotype to salivary secretion profiles. Selective breeding for enhanced therapeutic compounds remains unexplored.
- Density-reproduction mechanism: Sineva''s groups-vs-pairs effect never mechanistically explained. Pheromone signaling studies needed.
- Artificial diet optimization: No comparative studies of blood source (bovine vs. porcine vs. synthetic) on growth, salivary output, or efficacy.
- Batch variability: No studies quantifying variation in salivary compound profiles (hirudin, hyaluronidase) between batches or seasons.
- Accelerated maturation: 12–18 month cycle limits supply flexibility. Optimization of temperature, photoperiod, and feeding for faster cycles not systematically studied.
Quality Assurance & Regulatory
- Objective quality metrics: Current 6-point assessment is subjective. Quantitative metrics (spectrophotometric grading, force-displacement tone measurement) would improve reproducibility.
- Shelf-life validation: 30-day limit based on experience, not controlled studies. Salivary compound degradation time-course needed.
- Aeromonas surveillance: Batch culture and sensitivity testing recommended but not standardized. No published routine protocols.
- Aeromonas decolonization: No method to eliminate gut Aeromonas without killing the leech. Selective antimicrobial approaches could eliminate patient prophylaxis need.
- Cold-chain standards: No published temperature monitoring standards for leech shipping. Data-logging studies needed.
- Economic analysis: No cost-effectiveness comparison across FDA-cleared suppliers (purchase + shipping + DOA + storage).
The Standardization Imperative
Key Takeaways
Aquaculture & Quality Essentials
- 170+ years of captive breeding: From Brykov (1852) through Sineva (1944) to modern biofactories, the science of leech aquaculture has established reliable production of clinical-grade specimens.
- 12–18 month production cycle: From cocoon to clinical-ready leech. Supply chain disruptions require weeks to months to recover.
- 6-point quality assessment: Vigor, body tone, coloration, feeding readiness, intact integument, and appropriate size (3–10 cm). All six must pass before clinical use.
- Storage protocol: Dechlorinated water at 18–22°C, changed every 48 hours, glass jars with mesh lids, dark/dim environment, fed/unfed separation, daily viability checks.
- Environmental control is clinical quality control: Water chemistry (pH, hardness, temperature) directly determines leech phenotype and therapeutic quality (Garmash 2001).
Regulatory & Safety Essentials
- FDA 510(k) mandatory: Only Ricarimpex, Biopharm, and Carolina Biological are FDA-cleared. Non-cleared sources violate federal law.
- Single-use only: Each leech used on one patient, then destroyed in 70% ethyl alcohol. No reuse under any circumstances.
- OSHA BBP Standard applies: Written Exposure Control Plan required. Annual review mandatory. PPE: gloves, forceps, gowns, eye protection.
- Aeromonas is obligate, not avoidable: Every leech carries A. hydrophila / A. veronii. Prophylaxis (cipro + TMP-SMX) is mandatory, not optional. 2.4–20% infection rate without prophylaxis.
- Patients refusing antibiotics should not receive leeches: Per Mumcuoglu 2014, the risk-benefit ratio is unacceptable without prophylaxis.
Related Resources
Feeding Mechanism & Bite Dynamics
Triradiate jaw structure, bite biomechanics, blood extraction volumes, and attachment physiology.
Salivary Gland Secretion
Complete SGS compound catalog: hirudin, hyaluronidase, calin, destabilase, and 100+ bioactive molecules.
Aeromonas Management
Evidence-based prevention, surveillance, and treatment protocols for Aeromonas infections.
Clinical Protocols
Complete procedural guidelines from facility setup through post-procedure monitoring and follow-up.
Safety & Infection Control
Comprehensive safety framework: PPE, OSHA compliance, waste management, and institutional protocols.
Drug Interactions
Medication management including anticoagulants, NSAIDs, and antibiotic prophylaxis regimens.
FDA Regulatory Framework
510(k) classification, legal requirements, scope-of-practice considerations, and compliance guidance.
Taxonomy & Classification
<em>Hirudo verbana</em> vs. H. medicinalis, species identification, and taxonomic history.
Transparency & Trust
ASH editorial standards, sourcing, and how we handle uncertain claims.